Solitary Thyroid Nodule (STN) at DRHC Dubai
At Dr. Rami Hamed Center in DHCC, we provide the leading thyroid specialist in Dubai for complete care of thyroid diseases, including all diagnostic modalities and the latest non-surgical and surgical techniques available for the best outcomes
Definition:
A discrete swelling in an otherwise impalpable gland is termed a solitary thyroid nodule
- Prevalence: 3-5% of the adult population.
- Female: Male: 4:1
- The importance of STN lies in the risk of malignancy compared with other thyroid swellings.
- 10–15% of STNs are malignant.

Types of Solitary Thyroid Nodules (STN):
Workup of an STN History:
- Age and gender
- Children: A child with a thyroid nodule has a 50% chance of having a malignant
- Men > 50yrs
- Exposure to radiation for Hodgkin's Ca Breast
- Rapid nodule growth
- Pain, Hoarseness, Compressive symptoms
- History for specific endocrine disorders-medullary carcinoma, MEN type 2
- Family h/o thyroid carcinoma
Evaluation of STN:
- Lab Evaluation:
- Thyroid function test (T3, T4, TSH) - To identify patients with unsuspected hyperthyroid states and dictate appropriate workup.
- Serum calcitonin level-Medullary carcinoma is strongly suspected.
- Detection of thyroid autoantibodies in patients with toxic features (anti-microsomal and anti-thyroglobulin antibodies).
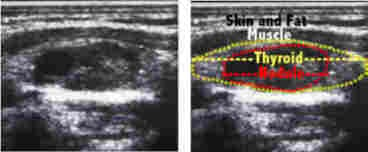
- Ultrasound:
- Nature of the swelling (Solid or cystic) – cystic lesions are usually but not always benign.
- To detect nodules of an MNG that are not clinically palpable.
- To detect lymph nodes.
- Follow-up of patients who are managed conservatively to detect increased volume of a suspicious lesion.
- Thyroid scan:
- Using Iodine131 or Technetium-pertechnetate 99m.
- On scanning, swellings are categorized as hot (overactive), warm (active), or cold (underactive)
- Not useful in distinguishing benign and malignant lesions since the majority of cold nodules are benign (80%), and some warm nodules are malignant (5%)
- The only indication is in patients with toxic features to differentiate Toxic adenoma (the rest of the gland is suppressed) from toxic MNG.

- FNAC:
- The single most useful investigation that can detect most conditions.
- A specimen is considered adequate if at least six properly prepared smears contain 15-20 groups of well-preserved clumps of follicular epithelium.
- Can diagnose colloid nodules, thyroiditis, papillary carcinoma, medullary carcinoma, anaplastic carcinoma, and lymphoma.
- Cannot distinguish between a follicular adenoma and carcinoma.
- Follicular cells in FNAC have a 6-20% chance of malignancy.
- Sensitivity – 89%
- Specificity - 91%
- False negative rate, 1- 6%. Hence, benign nodules diagnosed by FNAC should be followed sequentially with ultrasound to make sure the characteristics do not change.
- FNAC results – benign, suspicious, or malignant.
- Suspicious lesions increased the incidence of malignancy.
- MRI, CT (Rarely indicated)
- Only to evaluate retrosternal extension
- PET scan using FDGF18 (fluorodeoxyglucose F18)
- It can differentiate benign from malignant, but it is highly expensive and can not replace biopsy
Treatment options:
- Levothyroxine: (in benign nodule ) to keep TSH below 1 mU/L. It has many side effects, so not recommended.
- Surgery: indicated in
- FNAC positive or clinically suspicious (elderly, male, hard texture, fixed, recurrent laryngeal nerve palsy, lymphadenopathy, recurrent cyst)
- Cosmosis, Toxic nodules, and pressure symptoms
- Methods: Lobectomy + isthemicusctomy: In patients with low-risk factors and benign
- Total thyroidectomy: In patients with high-risk factors, Benign nodules, and malignant nodules
- Radioiodine: indicated in functioning nodules, contraindicated in pregnancy, lactation, and children. S/E: hypothyroidism, carcinogenic, fetal anomalies in pregnant women.
- Percutaneous ethanol injection and laser photocoagulation.
Guidelines:
According to the American Thyroid Association & American Association of Clinical Endocrinology:
- A radionuclide scan is only indicated in:
- suppressed TSH
- if FNAC → follicular neoplasia
- FNAC should be guided by U/S, especially if the nodule is partially cystic.
- Benign nodule → Life-long Follow-up every year (TSH, neck palpation, FNAC), if functioning: Iodine-131 is the TTT of choice, and surgery is indicated in:
- very large nodule, partially cystic, young patient, pregnant
- malignant nodule → surgery
- Autoimmune thyroiditis → cortison + L-thyroxin
- Infections → control
.png?width=281&height=59&name=bookanappointment%20(1).png)
Dubai Thyroid Clinic (DRHC) provides treatment for hypothyroidism, hyperthyroidism, thyroid cancer, thyroid disease, thyroidectomy, and thyroid surgery. To book your Appointment, please call +97142798200.




.webp?width=1080&height=1080&name=Doctor%20background%20For%20Website%20Dr.%20Fadi%20Nageeb%2009%20(1).webp)
.webp?width=1080&height=1080&name=Doctor%20background%20For%20Website%20Dr%20Abdul%20Majeed%20Khalid%20%2002%20(1).webp)



